- Normal right ventricular systolic function
- Normal left ventricular systolic function
- Two normal sized, well spaced papillary muscles
- PM = Posteromedial papillary muscle
- AL = Anterolateral papillary muscle
- Normal interventricular septal configuration (indicative of right ventricular systolic pressures less than 1/2 systemic)
- Normal thickness of the ventricular septum and posterior wall
- Zoomed up view of the ventricles
- Normal right ventricular systolic function
- Normal left ventricular systolic function
- Normal thickness of the interventricular septum
- Normal interventricular septal configuration (indicative of right ventricular systolic pressures <1/2 systemic)
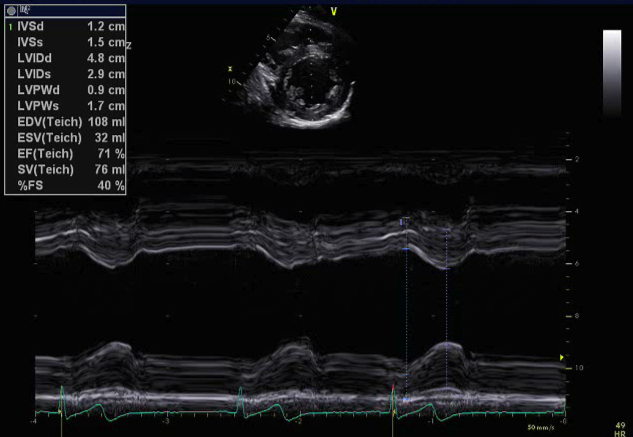
- M-mode moving image of the ventricles from a parasternal short axis view
- Values compared to reference normal values based upon patient’s body surface area
- Normal thickness of the interventricular septum and posterior wall
Fractional shortening (FS) is an MMode method. Measure left ventricular dimension by M Mode at end systole (LVESD) as well as end diastole (LVEDD). By entering your measurements in the following formula:
Fractional shortening: (LVEDD - LVESD / LVEDD) × 100
You will get the percentage of “size reduction” of the left ventricle. This is fractional shortening. This is not the same as ejection fraction (EF) as EF uses volumes.
Important: Fractional shortening and ventricular dimensions should only be quantified using m-mode in the setting of normal septal configuration.
- M-mode still frame measuring left ventricular thickness
- Values compared to reference normal values based upon patient’s body surface area
- Normal left ventricular interventricular septal and posterior wall thickness
Shortening Fraction (SF) is an M Mode method. M Mode provides measurements of the ventricle at end systole (LVESD) as well as end diastole (LVEDD). By entering your measurements in the following formula:
Shortening Fraction (SF) = (LVEDD - LVESD / LVEDD) × 100
You will get the percentage of “size reduction” of the left ventricle. This is shortening fraction. The value does not express ejection fraction because we are not computing volumes but distances (diameters).
Mean SF = 36% (range 28-45%)
Highest in early infancy (can range 35-45%)
Dependent on heart rate, contractility, preload and afterload
Conditions in which Shortening Fraction may be Inaccurate
- Wall motion abnormalities
- Pulmonary hypertension (septal flattening)
- Intraventricular conduction delay/bundle branch block
- Large pressure or volume loads on the heart
This view obtained from the parasternal short axis is an ideal view for profiling the right and left ventricle, assessing wall thickness and ventricular systolic function. M-mode measurements are obtained from this view.

- Transducer at left sternal border
- Notch pointed towards patient's left shoulder
- Probe angled inferiorly (tail up)
- Ventricular septal defects
- Right ventricular hypertrophy or dilation or dysfunction
- Left ventricular hypertrophy, dilation or dysfunction
- M-mode to quanitfy ventricle size and thickness and shortening fraction
- Trace left ventricle systolic and diastolic areas to calculate bullet ejection fraction
- Pressure and volume assessment
- Diastolic interventricular septal flattening
- Volume loaded right ventricle (atrial septal defect, pulmonary regurgitation)
- Systolic interventricular septal flattening
- Elevated right ventricular systolic pressures (pulmonary hypertension, pulmonary stenosis, VSD)
- Diastolic interventricular septal flattening
- Dyskinetic or paradoxical interventricular septal motion
- Previous surgical repair with VSD patch
- Mitral valve abnormality
- Single papillary muscle, closely spaced or hypoplastic papillary muscles